CBS News Correspondent Lilia Luciano asked Fauci if he’s concerned that bringing back the mask mandate “could erode trust in the efficacy of the vaccine?”
Fauci responded, “No, not at all. There are situations where one might want to go the extra mile to get the extra degree of protection.”
Treasury Secretary Janet Yellen said Friday the U.S. could return to lockdowns in areas of the country with low COVID-19 vaccination rates.
“We have solid rates of vaccination in many parts of the country. But certainly it’s something that could happen in areas where vaccination rates are low,” she told CNBC.
COVID-19 infections have risen in the U.S. recently after months of decline.
As of July, confirmed cases reached an average of 23,600 infections a day, according to Fox Business.
Yellen said that to prevent further lockdowns, it “is critically important that we maintain progress on vaccinating more Americans.”
VAERS data released today by the CDC showed a total of 463,457 reports of adverse events from all age groups following COVID vaccines, including 10,991 deaths and 48,385 serious injuries between Dec. 14, 2020 and July 9, 2021.
Los Angeles County Sheriff Alex Villanueva said his department would not enforce a COVID-19 health order mandating people to wear masks indoors, saying it’s “not backed by science” and citing an “underfunded” department.
The statement was issued one day after county officials announced a new mask mandate for residents in indoor public locations regardless of vaccine status, set to take effect Saturday at 11:59 p.m.
“Forcing the vaccinated and those who already contracted COVID-19 to wear masks indoors is not backed by science and contradicts the U.S. Centers for Disease Control and Prevention (CDC) guidelines,” Villanueva said Friday.
The CDC guidance states fully vaccinated people can resume daily activities without wearing a mask unless otherwise instructed by workplaces, businesses, or travel authorities.
Villanueva added deputies would “not expend our limited resources” to enforce the order, noting the Los Angeles County Sheriff’s Department is already “underfunded/defunded.” Still, the sheriff said law enforcement requests “voluntary compliance.”
Coronavirus patients who recovered from the virus were far less likely to become infected during the latest wave of the pandemic than people who were vaccinated against COVID, according to numbers presented to the Israeli Health Ministry.
Health Ministry data on the wave of COVID outbreaks which began this May show that Israelis with immunity from natural infection were far less likely to become infected again in comparison to Israelis who only had immunity via vaccination.
More than 7,700 new cases of the virus have been detected during the most recent wave starting in May, but just 72 of the confirmed cases were reported in people who were known to have been infected previously – that is, less than 1% of the new cases.
Roughly 40% of new cases – or more than 3,000 patients – involved people who had been infected despite being vaccinated.
With a total of 835,792 Israelis known to have recovered from the virus, the 72 instances of reinfection amount to 0.0086% of people who were already infected with COVID.
By contrast, Israelis who were vaccinated were 6.72 times more likely to get infected after the shot than after natural infection, with over 3,000 of the 5,193,499, or 0.0578%, of Israelis who were vaccinated getting infected in the latest wave.
According to a report by Channel 13, the disparity has confounded – and divided – Health Ministry experts, with some saying the data proves the higher level of immunity provided by natural infection versus vaccination, while others remained unconvinced.
Immigration agents have been informed by the Biden administration to be ready to process hundreds of thousands of migrant families and asylum claims in the coming months, The Washington Free Beacon is reporting.
A senior official told the outlet that the administration is expected to end Title 42, which is a law used by the Centers for Disease Control and Prevention under the Trump administration to keep migrants from entering the U.S.
Michigan’s Republican senators, who hold a majority in the state Senate, used a procedural method this week to support the repeal of a decades-old emergency powers law with a petition that cannot be vetoed by Gov. Gretchen Whitmer.
Michigan senators voted along party lines, 20-15, backing the petition to repeal the Emergency Powers of Governor Act of 1945, which was brought by the group Unlock Michigan and various people critical of Whitmer’s use of emergency powers during the COVID-19 pandemic.
Los Angeles County announced Thursday that it would re-instate an indoor mask mandate for residents, “regardless of vaccination status.”
The order, implemented after a rise in positive coronavirus cases in the county, will take effect Saturday at 11:59 p.m., according to L.A. County Health Officer Dr. Muntu Davis.
Maskless Democrat members of the Texas State Legislature smiled gleefully as they fled from Texas to Washington, DC, on Monday as part of their protest to halt the Texas GOP’s efforts to strengthen election safeguards in the Lone Star State.
Pictures show several smiling, maskless, Texas Democrats on a plane fleeing Texas in part of their move to protest the GOP’s efforts to strengthen election integrity in the state. Notably, Texas Democrats thwarted the effort at the end of the 2021 regular session by staging a walkout, leaving Republicans without a quorum to vote on the measure, Senate Bill 7, in May.
Everyone Who Gets the Jab Is Part of the Safety Trial
During that call, the Moderna representative reads her the following disclaimer:
“The Moderna COVID-19 vaccine has not been approved or licensed by the Food and Drug Administration, but it has been authorized for emergency use by the FDA under an emergency use authorization to prevent coronavirus disease 2019, for use in individuals 18 years of age and older.
There is no FDA-approved vaccine to prevent COVID-19. The EUA for the Moderna COVID-19 vaccine is in effect for the duration of the COVID-19 EUA declaration, justifying emergency use of the product unless that declaration is terminated or the authorization is revoked sooner.”
Scientists from University College London, and the Universities of York, Bristol and Liverpool say their studies of children are the most comprehensive yet anywhere in the world.
They checked England’s public health data and found most of the young people who had died of Covid-19 had underlying health conditions:
Around 15 had life-limiting or underlying conditions, including 13 living with complex neuro-disabilities
Six had no underlying conditions recorded in the last five years – though researchers caution some illnesses may have been missed
A further 36 children had a positive Covid test at the time of their death but died from other causes, the analysis suggests
Though the overall risks were still low, children and young people who died were more likely to be over the age of 10 and of Black and Asian ethnicity.
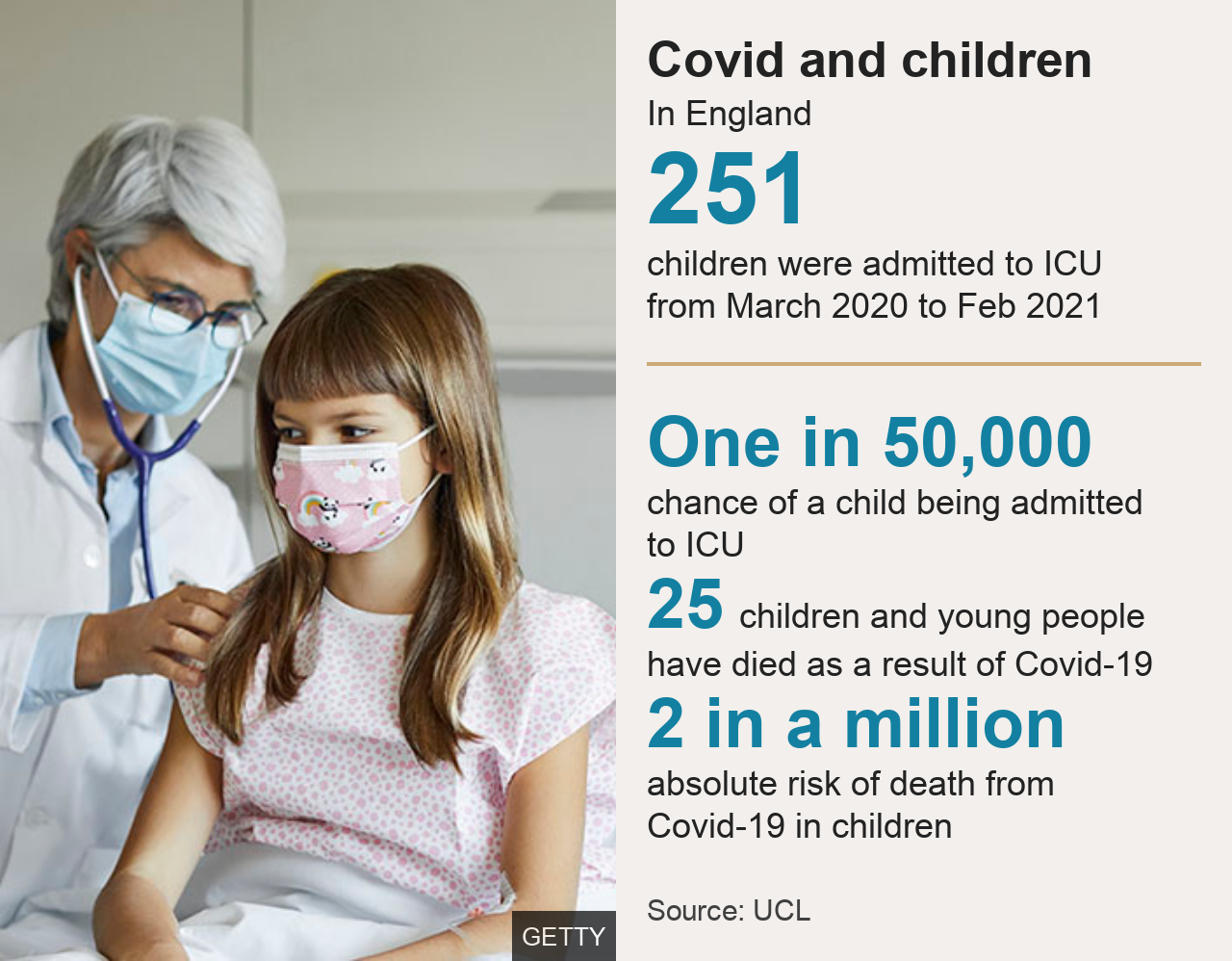
Researchers estimate that 25 deaths in a population of some 12 million children in England gives a broad, overall mortality rate of 2 per million children.
Current data shows some 128,301 people in the UK have died within 28 days of a positive coronavirus test since the pandemic started.
‘Hospital stays rare’
Separately, scientists considered all children and young people in England who had an emergency hospital admission for Covid up to February 2021:
Some 5,800 children were admitted with the virus, compared to about 367,600 admitted for other emergencies (excluding injuries)
About 250 required intensive care
There were 690 children admitted for a rare inflammatory condition linked to Covid, called paediatric inflammatory multisystem syndrome (PIMS-TS)
Though the absolute risks were still small, children living with multiple conditions, those who were obese, and young people with heart and neurological illnesses were most at risk
Lead researcher Prof Russell Viner said complex decisions around vaccinating and shielding children required input from many sources – not their work alone.
But he said if there were adequate vaccines, their research suggested certain groups of children could benefit from receiving Covid jabs.
He added: “I think from our data, and in my entirely personal opinion, it would be very reasonable to vaccinate a number of groups we have studied, who don’t have a particularly high risk of death, but we do know that their risk of having severe illness and coming to intensive care, while still low, is higher than the general population.”
He said further vaccine data – expected imminently from other countries, including the US and Israel – should be taken into account when making the decision.
Dr Elizabeth Whittaker, from the Royal College of Paediatrics and Child Health and Imperial College London, said it was encouraging they were seeing very few seriously unwell children in hospital.
She added: “Although this data covers up to February 2021, this hasn’t changed recently with the Delta variant. We hope this data will be reassuring for children and young people and their families.”
Europe, French researchers said they found traces of covid-19 in Nov 2019…scientists from National Cancer Institute of Milan and University of Siena found 10% of blood samples from a cancer screening trial contained COVID antibodies… samples included some from Sept 2019.
According to the study, 11.6% of individuals in a lung cancer clinical trial, months before the known COVID outbreak, had already been exposed to the virus. As antibodies take several weeks post infection to develop, it’s likely that some individuals had active infections in August 2019, or perhaps much earlier as antibody detection offers a minimum, not maximum, time window post-infection.
Early COVID antibodies were found not only in Italy but also in France, “Tests suggests COVID-19 could have existed in France in November 2019 – two months before the first cases were officially confirmed in Europe.”
Similar findings were described in the U.S. Antibody tests run on American Red Cross blood donations from December 2019 to January 2020 showed just over 1% of blood donations contained COVID-19 antibodies, suggesting that the virus was active in the U.S. in the fall of 2019, perhaps earlier.
Governor Andrew Cuomo (D-New York), who saw his poll numbers rise and scored a $5.1 million advance for his pandemic memoir, called leading the state (which had the worst response of all states) during the pandemic a “tremendous personal benefit.”
“Very few people were going through what we went through and we went through it together,” he said. “And speaking for myself, it was a tremendous personal benefit.”
However, unvaccinated individuals aboard the Freedom of the Seas do not have as many privileges as vaccinated guests, as Bloomberg detailed:
Jabbed guests, identified with special wristbands, get full run of the ship; those unprotected from the virus won’t even be able to walk into the sushi bar, casino, or spa.
…
Those with a hole punched in their SeaPass — indicating that they haven’t been jabbed or declined to show a vaccine card—will be segregated to one deck of the main dining room and will be banned from some of the better, more intimate for-a-fee dining venues. (That includes families with unvaccinated kids, too, so long as they’re sticking together.) Off limits will be the popular maritime-themed Schooner Bar pub and Viking Crown nightclub, the casino, art auctions, and the indoor Solarium pool and bar. Gatherings such as the 1970s-themed party will be open only to vaccinated guests. If you aren’t immunized and want to see a show, you’ll sit in a segregated area in the back of the theater. And you can only use the gym during specified hours.
Additionally, both vaccinated and unvaccinated guests must wear masks indoors when not eating and drinking, although Bloomberg adds that “some venues that are only open to vaccinated guests will be able to nix the rule.”
“The people who are not vaccinated don’t want restrictions,” Cruise Planners travel adviser Mindy Breitman said. “And the people who are vaccinated don’t want to wear masks because of the non-vaxed on board.”
Last month, two passengers aboard a “fully vaccinated” cruise ship, Celebrity Millennium, tested positive for the Chinese coronavirus.
“This is not complicated. We’re not asking anybody to make a political statement one way or another,” Fauci said during a segment of “All in with Chris Hayes” on MSNBC. “We’re saying, try to save your life, and that of your family, and that of your community.”
“We have so many things, as you said, so many diseases that I deal with that don’t have solutions,” Fauci continued. “It’s very frustrating. You don’t have a treatment, you don’t have a vaccine. Here we have a vaccine that’s highly, highly effective in preventing disease and certainly in preventing severe disease and hospitalization. It’s easy to get, it’s free and it’s readily available, so you’ve got to ask, what is the problem? Get over it. Get over this political statement and try to save the lives of yourself and your family.”
The government “absolutely” has the right to know citizens’ vaccination status, according to Health and Human Services Secretary Xavier Becerra.
“The federal government has spent trillions of dollars to try and keep Americans alive during this pandemic,” Becerra said Thursday on CNN, according to The Hill.
“So it is absolutely the government’s business, it is taxpayers’ business, if we have to continue to spend money to try and keep people from contracting COVID.”
When pressed whether the Biden administration would push to require proof for vaccinations, Becerra said states and local governments should decide that.
“The data shows that the medium age of death for Covid is often older than life expectancy,”
The medium age of death from Covid-19 in Ohio is 80 while the average life expectancy in the state is 73.
That means that people dying from Covid lived longer than one can expect to live in the state without getting the disease. He continued to show numbers from other parts of the country as well as the United Kingdom. All of the numbers, including the national numbers, showed that throughout 2020 the medium Covid-19-attributed death was higher than what an average person can expect to live.
Two counties in California have reviewed every COVID-19 fatality, refining the approach to classifying the cause of death. Santa Clara and Alameda County delineated those patients who died due to the illness progression of COVID-19 and those who tested positive at the time of death but were not symptomatic. This exercise reduced the number of COVID-19 deaths in both counties by nearly 25%.
Today the Journal JAMA Pediatrics published a study which looked at the impact of masks on children. The study was led by a researcher in Poland who was joined by six other doctors from Germany and Austria. The researchers concluded there was a significant build up of carbon dioxide in children using masks, to levels that are well beyond what is considered healthy for indoor air by the German government.
Fifty-seven authors from 17 countries have signed an endorsement urging that Covid-19 vaccinations be stopped unless new safety mechanisms are immediately implemented.
The authors include Dr. Peter McCullough, cardiologist and Vice Chief of Medicine at Baylor University Medical Center in Dallas, Texas, who has called for a halt to vaccinating 30-year olds due to “no clinical benefit” and safety concerns.
The petition to recall California Gov. Gavin Newsom has cleared its final hurdle on June 23 with confirmation from the state’s top election official that enough signatures remained after voters had been given a chance to withdraw support for the petition.
California Secretary of State Shirley Weber said 43 signatures have been withdrawn during a supplemental signature withdrawal period, leaving 1,719,900 verified signatures that still meet the threshold to initiate a recall election.
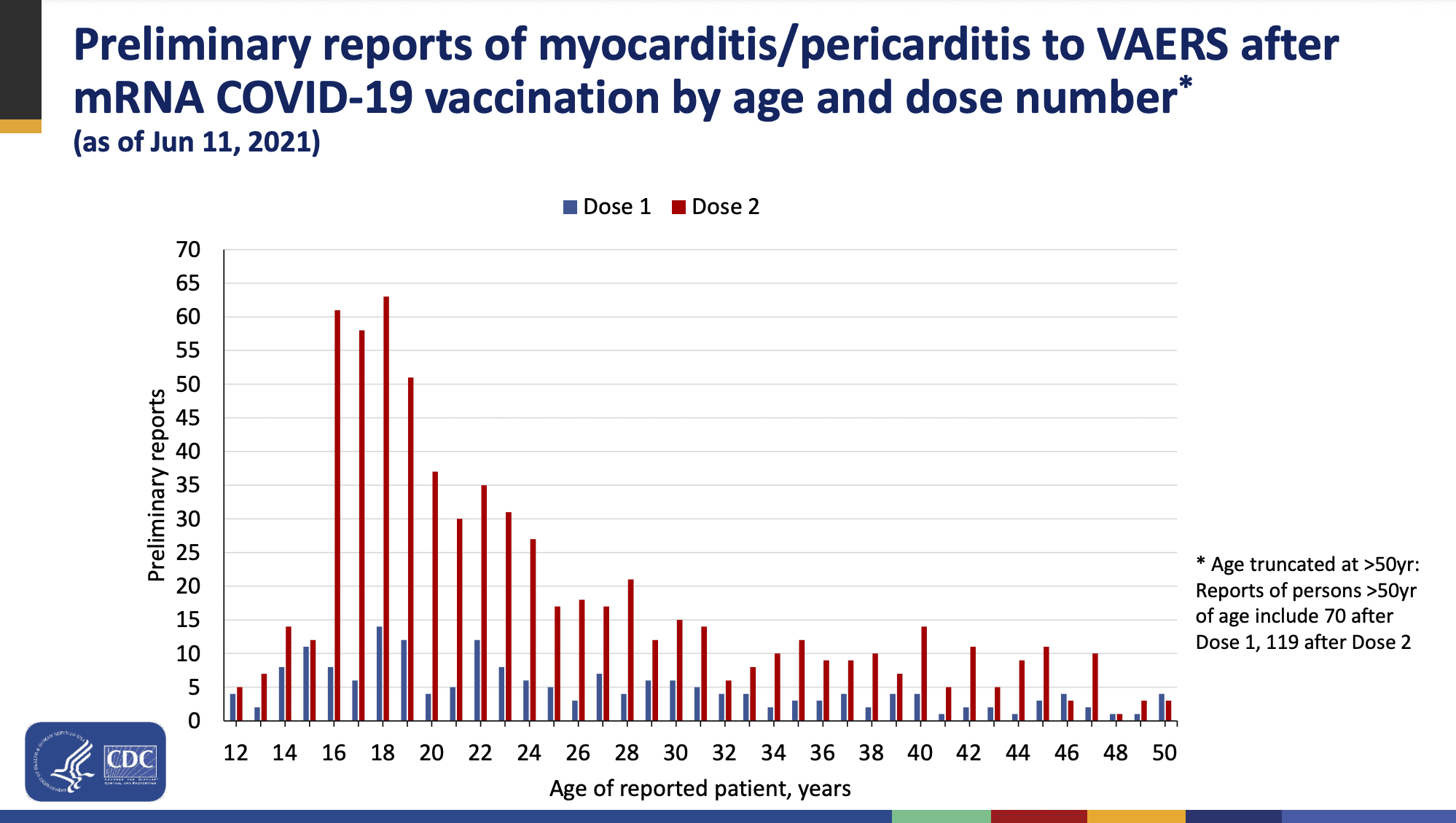
A CDC safety group said there’s a “likely association” between a rare heart inflammatory condition in adolescents and young adults mostly after they’ve received their second Covid-19 vaccine shot, citing the most recent data available.
There have been more than 1,200 cases of a myocarditis or pericarditis mostly in people 30 and under who received Pfizer’s or Moderna’s Covid vaccine, according to a series of slide presentations published Wednesday for a meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices.
Myocarditis is the inflammation of the heart muscle, while pericarditis is the inflammation of the membrane surrounding the heart.
“Clinical presentation of myocarditis cases following vaccination has been distinct, occurring most often within one week after dose two, with chest pain as the most common presentation,” said Dr. Grace Lee, who chairs the committee’s safety group. CDC officials are gathering more data to fully understand the potential risks, how to manage it and whether there are any long-term issues, she said.
The agency said there have been 267 cases of myocarditis or pericarditis reported after receiving one dose of the mRNA vaccines and 827 reported cases after two doses through June 11. There are 132 additional cases where the number of doses received is unknown, the CDC said.
Roughly 300 million of the shots had been administered as of June 11, the agency said.
“This is still a rare event,” Dr. Tom Shimabukuro said at the meeting. For both vaccines combined, there were 12.6 heart inflammation cases per million doses. The cases were more frequent among Moderna’s vaccine recipients at 19.8 cases per million versus eight cases per million for Pfizer’s, he said.
There is not yet enough evidence on the use of vaccines against COVID-19 in children to make recommendations for children to be vaccinated against COVID-19.
Children and adolescents tend to have milder disease compared to adults. However, children should continue to have the recommended childhood vaccines.
The election of 2020 is going to lay bare the dereliction of the Supreme Court for all to see. The COVD-19 pandemic gave numerous state election officials an excuse to implement far-reaching changes to our election processes. Those changes obviously made our systems vulnerable to fraud. States implemented massive mail-in balloting at the same time they relaxed ballot security and voter identification. They even extended the voting periods — to give the criminals more time to commit their fraud.
All these changes were unconstitutional. The Constitution clearly gives the various state legislatures the authority to define how their elections will be conducted — not state election officials. Election officials are only empowered to conduct elections within the rules set forth by their respective legislatures — except, apparently, during a pandemic. There must be a pandemic emanation hidden in a penumbra of the Constitution we didn’t know about. Alarmed that the changes would invite fraud, various organizations filed lawsuits to stop the changes.
The Supreme Court declined to get involved. It ruled that the plaintiffs lacked standing because nobody had been harmed — yet. Since the election hadn’t happened, nobody was damaged, and there was no case to be heard. They were thinking like a civil court, not the defenders of the Constitution they are sworn to be. It was a cowardly way to stay out of the political controversy. Unfortunately, it also missed an opportunity to defend the Constitution, which was clearly under attack.
After all the ad-hoc changes had been allowed to stand, the election of 2020 saw an unprecedented number of irregularities — too many to ignore. Election observers were banned from observing the election. Counting stopped in the middle of the night and then restarted after boxes of ballots were mysteriously found. There are reports of ballots being driven across state lines — by the truckload. There were even precincts that counted more ballots than there were registered voters! A number of states filed lawsuits against the states in which these irregularities occurred.
Even though the Supreme Court is supposed to be the arbiter of cases between states, it again refused to get involved. They ruled that Texas couldn’t sue Pennsylvania because Texans had their votes accurately counted and therefore were not harmed by Pennsylvania. Apparently having the wrong president crammed down the throats of Texans is not considered “harm.” Given the flood of illegal aliens President Asterisk has invited — and the crime that has accompanied them — would the justices consider Texas “harmed” now?
A number of other cases were dropped because the court considered them “moot.” The election had been certified and nothing was going to change that — hence no need to look at the evidence. In the immortal words of Hillary Rodham Clinton, “At this point what difference does it make?”
The court seems to have three distinct voting blocs:
The oath keepers — These are the justices that are willing to stand up and defend the Constitution even if it means they’ll have to endure attacks. Justices Thomas, Alito, and Gorsuch make up this bloc.
The jellyfish — These are the justices that lack the spine to face controversy. They’re more concerned about defending the court than the Constitution. Justices Roberts, Barrett, and Kavanaugh make up this bloc.
The subversives — These are the justices that have been using penumbras and emanations to rewrite the constitution in pursuit of social engineering. Justices Kagan, Sotomayor, and Breyer make up this bloc.
It’s rumored that only three justices wanted to hear the 2020 election lawsuits. Does anyone doubt that it was those who comprise the “oath keepers” bloc?
Now, Chief Justice Roberts has placed his court in a trick-box. By choosing to stay out of the election controversy, John Roberts has bet the court’s reputation that the mysteries of the election would remain mysteries. As wagers go, it was not a particularly smart one. The election involved millions of ballots, tens of thousands of election workers, and thousands of counties. If there was fraud, there is too much evidence, in too many hands, to stay hidden.
Tellingly, the Democrats are scrambling to keep the truth hidden, but it’s slowly coming out. State sponsored forensic audits, as well as private investigations, are turning over the stones. We’ll likely know the truth by the end of this year. If it turns out that the election was stolen, the Supreme Court will be exposed as derelict, weak, and useless. It will all be because the jellyfish bloc doesn’t understand the psychology of bullies.
The Supreme Court avoided involvement in the election because they wanted to stay out of the controversy — they didn’t want to be bullied by the Democrats or the media. There are other possible motives, but they’re even more disturbing. Cowing to bullies will not avoid conflict. Bullies prey on weakness. One has to either stand up to them eventually or accept servitude. Every kid on the playground has learned that lesson by the 8th grade. Apparently, John Roberts hasn’t. Each time Chief Justice Roberts has acceded to the bullies, he’s made the court’s future challenge greater.
Ruling that last minute ad-hoc election changes were unconstitutional would have been relatively straightforward — but the court didn’t. Hearing the election fraud evidence and adjudicating the result would have created a political crap-storm — but it would have been the right thing to do. What will become of the court’s reputation if it becomes obvious that the election was stolen and rather than stand up, it sat down?
An April poll by Rasmussen Reports found that 51% of the population believes that fraud affected the election outcome. Does Roberts grasp the significance of that number? It’s the percentage of the population who believe the Supreme Court was derelict in defending the Constitution. If John Roberts wanted to defend the court, perhaps he should have considered pursuit of the truth rather than avoidance of controversy.
A recent Ipsos poll found that 63% of the public thinks it’s time to impose term limits on Supreme Court Justices. The public isn’t stupid. It recognizes that the Supreme Court needs to be taken to the woodshed. The next few months will say a lot about the Supreme Court. Will it correct course, or will it embrace servitude to the mob?
John Green is a political refugee from Minnesota, now residing in Star Idaho. He is a retired engineer with 40 years of experience in the areas of product development, quality assurance, organizational development, and corporate strategic planning. He currently writes at the American Free News Network (americanfreenewsnetwork.org).
He can be followed on Facebook or reached at greenjeg@gmail.com.
15 DAY SLOW THE SPREAD= 15 MONTH LOCKDOWN-SHUTDOWN
Michigan Gov. Gretchen Whitmer on Thursday announced that all statewide restrictions put in place to curb the transmission of COVID-19 would come to an end on June 22—more than a week ahead of schedule.
A recent poll showed that 55% of voters prefer a “generic Republican” to Stretchin’ Gretchen in the next election.
“At the time, it was scarier to be associated with Trump and to become a tool for racists, so people didn’t want to publicly call for an investigation into lab origins,”said Alina Chan in an interview with NBC News.
Chan is a postdoctoral associate at the Broad Institute of MIT and Harvard University who specializes in genetic engineering.
On its website, NBC titled its Wednesday story about the interview “The science around the lab leak theory hasn’t changed. But here’s why some scientists have.”
NBC wrote:
Chan said there had been trepidation among some scientists about publicly discussing the lab leak hypothesis for fear that their words could be misconstrued or used to support racist rhetoric about how the coronavirus emerged. Trump fueled accusations that the Wuhan Institute of Virology, a research lab in the city where the first Covid-19 cases were reported, was connected to the outbreak, and on numerous occasions he called the pathogen the “Wuhan virus” or “kung flu.”
NEW YORK — Gov. Andrew Cuomo says New York is finally ready to reopen amid the COVID-19 pandemic.
The governor announced during a news conference Tuesday that New York reached the 70% threshold for vaccinations in eligible people 18 and older.
“We can now return to life as we know it,” the governor said Tuesday.
Under the reopening, state mandates related to COVID will be relaxed effective immediately. This includes capacity and social gathering restrictions, as well as health screening regulations.
An Ohio college student died about two weeks after receiving her second dose of the Moderna mRNA COVID vaccine.
19-year-old Northwestern University freshman Simone Scott passed away from pneumonia complications Friday following a heart transplant she received as a result of myocarditis-induced heart failure last month.
Scott’s parents, left without an official explanation from doctors how this happened, believe the Moderna vaccine played a role in their daughter’s death, according to investigative reporter Alex Berenson.
“My fear is that we’ll never know what happened to Simone,” her father, Kevin Scott, reportedly said Sunday night. “[The vaccine] is a coincidence that is too big to ignore.”
On Monday’s broadcast of ABC’s “Good Morning America,” ABC News Senior National Correspondent Terry Moran reported that one of the scientists who signed a letter in the medical journal The Lancet that dismissed the theory that COVID-19 came from a lab now believes the lab leak theory is more probable, and “several” other signatories of the letter are now unsure that the virus came from nature.
The number of small businesses in America has declined by nearly 40% since the lockdowns began last year, including more than half the leisure and hospitality industry.
And things are actually starting to get worse again. A separate poll shows another 35% of small businesses say they are at risk of closing permanently by the end of this summer due to inflationary pressures, rising gas prices, and increasing labor shortages.
The Wisconsin Supreme Court has ruled against the city of Madison’s public health agency in a dispute over the power to close schools during the pandemic.
A top city health official decried Friday’s decision, saying it would put children at risk.
“The Wisconsin Supreme Court ruled that local health officers cannot close schools within their jurisdictions. We are extremely disappointed in the court’s decision, which has much further reaching implications than just this current pandemic,” health director Janel Heinrich said.. “This decision hinders the ability of local health officers in Wisconsin to prevent and contain public health threats for decades to come.”
A panel of the 1st District Court of Appeal, in a 2-1 decision, said Alachua County Circuit Judge Donna Keim did not properly consider the privacy rights of plaintiff Justin Green before she rejected a request for a temporary injunction against the mask requirement.
“The trial court simply looked at the right asserted by Green too narrowly, relying on the wrong privacy jurisprudence,” said the 13-page majority opinion, written by Judge Adam Tanenbaum and joined by Judge Robert Long. “The right to be let alone by government does exist in Florida, as part of a right of privacy that our (Florida) Supreme Court has declared to be fundamental. … (The Supreme Court) has construed this fundamental right to be so broad as to include the complete freedom of a person to control his own body. Under this construction, a person reasonably can expect not to be forced by the government to put something on his own face against his will. Florida’s constitutional right to privacy, then, necessarily is implicated by the nature of the county’s mask mandate.”
The majority stopped short of declaring the Alachua County requirement unconstitutional but sent the case back to the lower court for reconsideration.
Emergency room (ER) mental health visits increased 31% among children aged 12-17 years old in 2020 compared to the previous year, according to a Centers for Disease Control and Prevention (CDC) report released Friday. The CDC noted that, while it couldn’t definitively establish a cause, it’s likely that pandemic-related restrictions on everyday life could be to blame for the increase.
“Young persons might represent a group at high risk because they might have been particularly affected by mitigation measures, such as physical distancing (including a lack of connectedness to schools, teachers, and peers); barriers to mental health treatment; increases in substance use; and anxiety about family health and economic problems,” the report stated.
“Previous studies have claimed that shelter-in-place orders saved thousands of lives, but we reassess these analyses and show that they are not reliable.
We find that shelter-in-place orders had no detectable health benefits, only modest effects on behavior, and small but adverse effects on the economy.
To be clear, our study should not be interpreted as evidence that social distancing behaviors are not effective. Many people had already changed their behaviors before the introduction of shelter-in-place orders, and shelter-in-place orders appear to have been ineffective precisely because they did not meaningfully alter social distancing behavior.”
It is now unanimous, and I have been proven right (once again) that the initial World Health Organization Report on the Wuhan Lab was flawed and must be redone, this time by a truly transparent investigation.
We were right about the China Virus from the beginning, and now the entire world sees it. This is why the Chinese Communist Party should pay $10 Trillion in global reparations for what they allowed to happen, the worst event in world history.
Even here in the United States, the so-called experts like Dr. Fauci were wrong about the Wuhan Lab and China’s role the entire time.
Just think how bad things would have gotten if I followed Dr. Fauci’s advice and never closed down travel from China (and other things)?
Dr. Fauci likes to say that he is “science,” when in fact he is merely science fiction!
It is “time to distinguish” between the freedoms afforded to those who have been vaccinated against the Chinese coronavirus and those who haven’t, said former British prime minister Tony Blair.
Dozens of studies show that lockdowns were an ineffective pandemic response. The list just got longer.
In May, Youyang Gu, an MIT-trained engineer and data scientist, released data showing that government restrictions were not correlated with lower COVID mortality in America. Government restrictions were correlated with higher unemployment, however.
Going outdoors mask-free is not an example of a risky activity, regardless of vaccination status, because the transmission rate in most outdoor settings is extremely low — far lower than the 10% rate the CDC reported.
Dr. Anthony Fauci said in a private email that “most transmissions” of virus “occur from someone who is symptomatic” and “not asymptomatic.” However, Fauci publicly touted the idea that asymptomatic spread is “not rare” but in fact common, as the medical experts spread fear about the virus. (RESEARCH: CDC Inflated COVID Death Count By At Least 1600 Percent). In a February 2020 email, Fauci wrote, “Error in my statement to you. I meant to say that “……most transmissions occur from someone who is symptomatic” — not asymptomatic. I am really tired. Not much sleep these days. Best, Tony.” However, in June 2020 Fauci said that asymptomatic transmission of Coronavirus is not rare, even chastising another expert for downplaying asymptomatic spread. Fauci said, “We have experience here with people who are without symptoms that cause us to believe that the transmission from an asymptomatic person to someone who’s not infected is not a rare event…But it’s becoming pretty clear to us that one cannot say that it is rare. It is likely not rare.”
Former White House COVID-19 testing czar, Adm. Brett Giroir, has accused Dr. Anthony Fauci of lying last year about the origins of the CCP virus, as health officials ramp up efforts to probe the hypothesis that the virus emerged from a lab accident.
In May last year, Fauci, the director of the National Institute of Allergy and Infectious Diseases (NIAID), claimed that the virus could not have been “artificially or deliberately manipulated” at China’s Wuhan Institute of Virology (WIV)—a possibility that is now receiving wider recognition.
German Study Finds Lockdown ‘Had No Effect’ on Stopping Spread.
A major new study by German scientists at Munich University has found that lockdowns had no effect on reducing the country’s coronavirus infection rate.
Oh.
“Statisticians at Munich University found “no direct connection” between the German lockdown and falling infection rates in the country,” reports the Telegraph.
The study found that, on all three occasions before Germany imposed its lockdowns in November, December and April, infection rates had already begun to fall.
The R rate – the number that indicates how many other people an infected person passes the virus to – was already under 1 before the lockdown restrictions came into force.
As we highlighted last year, a leaked study from inside the German Ministry of the Interior revealed that the impact of the country’s lockdown could end up killing more people than the coronavirus due to victims of other serious illnesses not receiving treatment.
This is by no means the only study to have concluded that lockdowns are completely useless and don’t work.
A peer reviewed study published in January by Stanford researchers found that mandatory lockdowns do not provide more benefits to stopping the spread of COVID-19 than voluntary measures such as social distancing.
Back in March, Stanford medical professor Dr. Jay Bhattacharya told Newsweek that COVID-19 lockdowns are “the single worst public health mistake in the last 100 years.”
Earlier this year, academics from Duke, Harvard, and Johns Hopkins concluded that there could be around a million excess deaths over the next two decades as a result of lockdowns.
Other research has concluded lockdowns will conservatively “destroy at least seven times more years of human life” than they save
Fauci sent an urgent email to Hugh Auchincloss, the NIAID Principal Deputy Director. It reads: “Hugh: It is essential that we speak this AM. Keep your cell phone on. I have a conference call at 7:45 AM with Azar. It likely will be over at 8:45 AM. Read this paper as well as the e-mail that I will forward to you now. You will have tasks today that must be done. Thanks, Tony”
The same day, he recieved a reply from Auchincloss. It reads: “The paper you sent me says the experiments were performed before the gain of function pause but have since been reviewed and approved by NIH. Not sure what that means since Emily is sure that no Coronavirus work has gone through the P3 framework. She will try to determine if we have any distant ties to this work abroad.”
Oklahoma Gov. Kevin Stitt (R) issued an executive order Friday that bans state agencies from enforcing mask mandates and coronavirus vaccine requirements for people using their buildings.
– a patchwork of mask mandates by local government is NOT the way to govern. Just like a patchwork of different GUN LAW is not, either. State law preemptions are perfectly consistent with the constitution.
Idaho’s governor on Friday repealed a mask mandate ban that was implemented while he was away on a trip.
The state’s lieutenant governor, Janice McGeachin, a Republican who is running for governor, issued an executive order the day prior barring local governments from requiring masks be worn. She did so with the authority she had as acting governor because Gov. Brad Little, a Republican, was out of state.
Actor Matthew McConaughey, who is weighing a gubernatorial bid in the state of Texas, is going to bat for universal mask wearing, expressing his belief that it does not take away an individual’s identity or freedom and asserting that no data exists showing the practice as harmful.
“I’m not believing you’re really scared of this little cotton thing. I don’t really feel that takes away your identity and your freedom,” the Gentleman star said during an appearance on The Carlos Watson Show.
“There’s no data that says it’s not a good thing. No data that says it’s harmful,” he continued, asking everyone to “take one for the team here.”
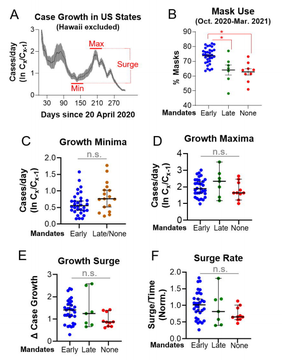
Our main finding is that mask mandates and use are not associated with lower SARS-CoV-2 spread among US states. 80% of US states mandated masks during the COVID-19 pandemic. Mandates induced greater mask compliance but did not predict lower growth rates when community spread was low (minima) or high (maxima). We infer that mandates likely did not affect COVID-19 case growth, as growth rates were similar on all days between actual or modeled issuance dates and 6 March 2021. Higher mask use (rather than mandates per se) has been argued to decrease COVID-19 growth rates…. Higher mask use did not predict lower maximum growth rates, smaller surges, or less Fall-Winter growth among continental states. Mask-growth rate correlation was only evident at minima. This may be an artifact of faster growth at fewer normalized cases, as well as regional differences in case prevalence early in the pandemic. States in the high mask quintile grew at similar rates as states in the low mask quintile after maxima (when interstate total case differences were smaller than before minima).
Principal Dr. Ira Pernick said students are required to show proof of coronavirus vaccination to attain facial freedom, the paper said. Unvaccinated students will also have to produce a negative coronavirus test in order to participate.
Port Washington High School’s prom is scheduled to be held June 27 and “kids who are vaccinated will be able to attend maskless — while those who aren’t will need to wear a face covering,” the New York Post reported.
A veto-proof majority of Michigan representatives passed a bill Tuesday that would require the state to refund coronavirus-related fines after Gov. Gretchen Whitmer (D) was caught violating her own order.
By a 74-34 vote, the state House swiftly passed HB 4501, a bill brought up for consideration after Breitbart News busted Whitmer for violating her restaurant table capacity order last weekend.
“If the governor can violate her orders without any repercussions, then why should our business owners be fined,” state Rep. Steve Johnson (R) wondered.
New findings reported Tuesday in a University of Louisville study challenge what has been the prevailing belief that mask mandates are necessary to slow the spread of the Wuhan coronavirus. The study notes that “80% of US states mandated masks during the COVID-19 pandemic” and while “mandates induced greater mask compliance, [they] did not predict lower growth rates when community spread was low (minima) or high (maxima).” Among other things, the study—conducted using data from the CDC covering multiple seasons—reports that “mask mandates and use are not associated with lower SARS-CoV-2 spread among US states.”
A Sunday school teacher was arrested at Thursday night’s Timberlane Regional School Board meeting moments after she and several other unmasked attendees showed up to demand an end to a school mask mandate.
The meeting was planned to be held in person at the district’s Performing Arts Center, but board Chairwoman Kimberly Farah quickly shut it down before it began and required that it be held remotely.
“I didn’t want to jeopardize the health of the staff and the students,” Farah said as several Plaistow police officers and state police troopers swarmed inside and outside the auditorium.
The abrupt end to the 7 p.m. in-person meeting happened shortly after Atkinson resident Jackie Wydola watched as police arrested her mother, Kate Bossi, when they entered the building without masks as required by school policy.
“You are violating my rights right now. You are remiss,” Bossi told Sgt. Alec Porter as she was being arrested.
“Come on Sgt. Porter, you know this is wrong what they’re doing to our kids,” one man shouted during the arrest.
“Are you seriously doing this you guys. This is law enforcement. You’re not enforcing laws, you’re enforcing policy. That doesn’t matter,” Wydola told officers.
Wydola said that before the arrest her mother “didn’t really have any interaction with the officer. She just walked into the building, and when they realized that she had come into the auditorium they followed her in here.”
She said her mother was the first unmasked person to walk into the building.
Porter declined to comment on the reason for the arrest at the scene, but Wydola, who identified Bossi, said she was told that her mother was arrested for disorderly conduct.
At the heart of the conflict is Board Chairwoman Kimberly Farah, a mini-tyrant who flexes her power over children This evil totalitarian is said to “strut around” reminding people she was in the military and doesn’t need to listen to the concerns of the parents who are there to serve her.
When asked if she felt threatened after the in-person meeting ended, Farah responded, “No, I was in the Army. I do not. I’m quite confident in the fact that I’ve got backups here.”
The arrest and mask mandates are said to be there to protect the children from a disease that is less of a threat to them than the flu. People like Kimberly Farah prop themselves up on the ignorance and fear of others.
“The Constitution of the United States is a law for rulers and people, equally in war and in peace, and covers with the shield of its protection all classes of men, at all times and under all circumstances. No doctrine involving more pernicious consequences was ever invented by the wit of man than that any of its provisions can be suspended during any of the great exigencies of government.” — Ex Parte Milligan, Supreme Court of the United States, 1866.
Three Republican lawmakers will be fined $500 each for entering the House floor without masks, despite the latest guidance from the Centers for Disease Control and Prevention (CDC).
“A Capitol official said that Republican Reps. Brian Mast (Fla.), Beth Van Duyne (Texas) and Mariannette Miller-Meeks (Iowa) will be fined $500 after ignoring previous warnings,” The Hill reported.
“Seven other Republicans will be issued formal warnings and would face $500 fines if they refuse to wear masks on the House floor again: Reps. Thomas Massie (Ky.), Marjorie Taylor Greene (Ga.), Lauren Boebert (Colo.), Chip Roy (Texas), Bob Good (Va.), Mary Miller (Ill.), and Louie Gohmert (Texas).”
For the next offense, the three offenders will be fined $2,500.
Hospital Pediatrics,” a journal of medicine for pediatric care, published two research papers Wednesday that found child hospitalizations for COVID-19 were over-counted by at least 40% in the state
“Hospital Pediatrics,” a journal of medicine for pediatric care, published two research papers Wednesday that found child hospitalizations for COVID-19 were over-counted by at least 40% in the state, and researchers believe it’s likely national numbers were similarly inflated. New York magazine reported commentary from Dr. Monica Gandhi, an infectious disease specialist at the University of California, San Francisco, and her colleague Amy Beck, an associate professor of pediatrics, that explained the studies’ findings.
“Taken together, these studies underscore the importance of clearly distinguishing between children hospitalized with SARS-CoV-2 found on universal testing versus those hospitalized for COVID-19 disease,” they wrote. The reported hospitalization rates “greatly overestimate the true burden of COVID-19 disease in children.” In an interview, Gandhi told New York magazine “there is no reason to think these findings would be exclusive to California. This sort of retrospective chart review will likely reveal the same findings across the country.”
New York magazine summarized the key findings from the two studies:
In one study, conducted at a children’s hospital in Northern California, among the 117 pediatric SARS-CoV2-positive patients hospitalized between May 10, 2020, and February 10, 2021, the authors concluded that 53 of them (or 45 percent) “were unlikely to be caused by SARS-CoV-2.” The reasons for hospital admission for these “unlikely” patients included surgeries, cancer treatment, a psychiatric episode, urologic issues, and various infections such as cellulitis, among other diagnoses. The study also found that 46 (or 39.3 percent) of patients coded as SARS-CoV2 positive were asymptomatic. In other words, despite patients’ testing positive for the virus as part of the hospital’s universal screening, COVID-19 symptoms were absent, therefore it was not the reason for the hospitalization. Any instance where the link between a positive SARS-CoV2 test and cause of admission was uncertain the authors erred toward giving a “likely” categorization.
In the second study, at the fifth-largest children’s hospital in the country, out of 146 records listing patients as positive for SARS-CoV-2 from May 1, 2020, to September 30, 2020, the authors classified 58 (40 percent) as having “incidental” diagnosis, meaning there was no documentation of COVID-19 symptoms prior to hospitalization. Like the first study, and as has been typical around the nation, this hospital implemented universal testing of inpatients for SARS-CoV-2. An example of incidentally SARS-CoV-2-positive patients are those who came to the hospital because of fractures. Patients who may have had COVID-19 symptoms but who had a clearly documented alternative reason for them, such as a child with abdominal pain and fever found to be related to an abdominal abscess, were also deemed to have incidental diagnosis. The study categorized 68 patients, or 47 percent, as “potentially symptomatic,” which was defined as when “COVID-19 was not the primary reason for admission for these patients, and COVID-19 alone did not directly require hospitalization without the concomitant condition.” Examples of these patients were those with acute appendicitis, since that condition includes gastrointestinal symptoms that may also present in COVID-19.
Figures attest to a phenomenon some have termed “mask dependency”: Mask production rose 20 per cent year on year in 2015, to a record high of 4.9 billion pieces, according to latest data from the Japan Hygiene Products Industry Association.
Dr. Anthony Fauci supports businesses choosing to leave mask mandates in place because the “issue,” he said, is that “we don’t have any way of knowing who is vaccinated.”
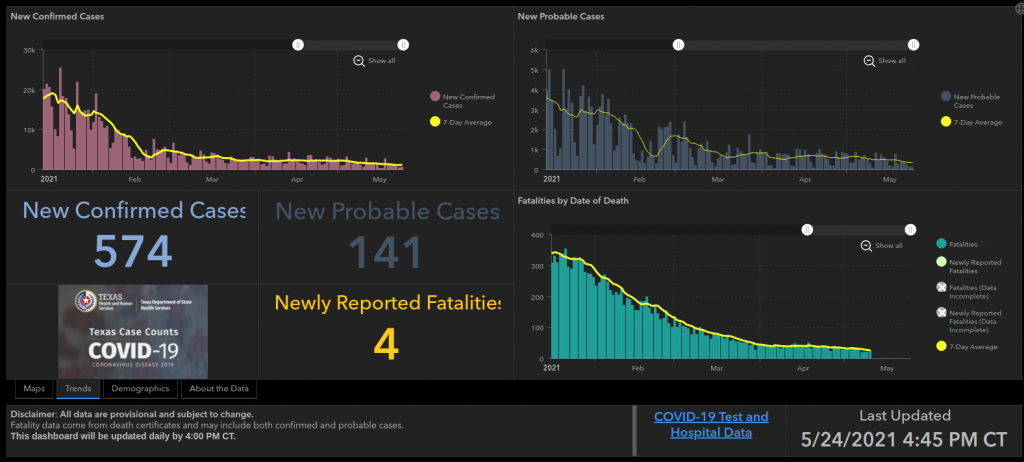
Over the weekend, Texas reported reaching the milestone of zero deaths from COVID-19 for the first time since March 2020. Arizona, Minnesota, and Massachusetts also recently reported COVID death-free days for the first time in months.